When I choose to explain to someone that I have declined to take the COVID jabs, I am often met with an expression of surprise, or one of anger. Then, when the inevitable question “Why?” is posed, my answer cannot be distilled into a ten second response. This blog article is intended to explain my choice, partly to give me a simple way to respond to the “Why?” question, and partly to help me distil my views on the evolving COVID jab debate. Prior to October 2020 I knew little, if any, of the information outlined below — building the knowledge gradually while I researched and sought to figure out what choice to make about COVID jabs. I have tried to give references and links to the sources of the information where possible. I have also tried to avoid the trap of cherry-picking, which is where only the data, facts and information that support my views, are included. If you read this and spot ommissions where I appear to have fallen into the trap and have not given relevant alternative information, please tell me and the article will be amended. Much of the data referenced here is for the UK, and much comes from the UK Health Security Agency (UKHSA), the successor organisation to Public Health England.
Sections 1-4 (see Contents below) are there to establish a base set of information to make it possible to then understand what is covered in sections 5-9. The article is not short, but then, the topic is not trivial.
UPDATE: I’m in the process of adding some more content on the back of feedback gratefully received from a few folks. This includes some analysis on NHS impacts, vaccine impacts, and some thoughts about what I think would have been a better approach for policy during the pandemic.
Contents
- Vaccines – the early days
- Our immune system
- Viruses 101
- Vaccines 101
- What do the COVID jabs do (and not do)?
- Making vaccines is difficult…
- Exploring some data, busting some myths
- My decision to decline the jabs
- Closing thoughts
- Addendum: More analysis and hypotheses
References
1. Vaccines — the early days
Efforts to create immunity from infection and disease date back thousands of years with Chinese, South Asian and African examples recorded of people exposing themselves to preprations derived from smallpox infections, a practice that was called inoculation. This practice reached European and American lands in the 1700s, where it was also called variolation, after the Latin name for smallpox—variola.1
Then, in the late 1700s, Edward Jenner undertook a set of trials and experiments as he attempted to find to find a way to prevent smallpox. His efforts earned him a place in history as the father of immunology. He is said to have observed that maids in dairy parlours often claimed to be immune from smallpox due to the fact that they had prior infections from cowpox, a related virus. Jenner surmised that immunity developed from cowpox infection would protect against smallpox infection, and to test his hypothesis, he took cowpox scabs and puss from the infection on the arm of a dairy maid called Sarah Nelmes and then applied this into an open cut on the arm of James Phipps, a healthy 8-year old boy (and son of his gardener). James became ill for a short period from cowpox and then recovered. Jenner then subsequently introduced smallpox scabs and puss into the arm of James, and observed that James did not become ill with smallpox.
After further trials Jenner then declared, in 1796, that he had discovered a method for inoculation against smallpox, and he named the process vaccination, possibly drawing on the Spanish word ‘vaca’, for cow.2
After Jenner
Jenner’s method of vaccination was in fact somewhat distinct and different to the established vaccination methods used today. Jenner’s method required vaccination with one virus, cowpox, to protect against a different virus, smallpox. It wasn’t until the late 19th century, when Louis Pasteur undertook experiments to explore for ways to prevent anthrax infection, that vaccination using a weakened version of the same pathogen was established.
Pasteur discovered micro-organisms in the blood of persons suffering from anthrax. He developed a solution containing a weakened form of the bacteria, which he could use as an inoculating agent, and was able to measure the success of his experiment by the absence of bacteria in the inoculated host. Pasteur named this inoculation process vaccination, in honour of Jenner’s work on Smallpox, and this became the generic term for the technique.3
Revisiting Jenner and smallpox…
If you undertake some research into vaccination history, and in particular vaccination against smallpox, you would almost certainly come away with a narrative that Jenner’s discoveries were pioneering and ground-breaking, and paved the way for a global vaccination programme that ultimately resulted in the complete eradication of smallpox in the wild (laboratory-stored quantities of the virus continue to exist). Indeed you may, like me, recall learning during childhood about the miracle of Jenner’s work and discoveries, lauding him as such a pioneer. Dig a little deeper however, and that simple narrative crumbles. Jenner was far from being a creditable scientist, practising with honesty and integrity. Jenner’s claims that immunity developed from prior cowpox infection protects against smallpox were rubbished, both by vast reams of empirical evidence from other physicians who testified of numerous examples of smallpox disease in subjects who had prior cowpox infections, but also by numerous recordings of smallpox infections following vaccination!4 When Jenner first introduced his thesis to the Royal Society, it was rejected, and indeed Jenner himself was ridiculed by many of his peers. While neither of these facts should be considered evidence that Jenner’s theories were unfounded, the evidence and data from decades of smallpox vaccination efforts from 1796 to the early 1900s suggests that smallpox vaccination in many sitations killed as many people as smallpox itself5, and causal links between vaccination and infection reduction and disease reduction were never established. Perhaps the most notable event during that period was the experience of Leicester between 1880 and 1908. With a compulsory national smallpox vaccine in place, following an outbreak, the people of Leicester voted out of power their town council and the new council abolished compulsory vaccination and instead created a smallpox safety system: laws were passed which made vaccination voluntary, a rapid notification and quarantine system was established, including specially trained personnel and comfortable quarantine facilities for anyone exposed to the index (initial) case. The method, known as the “Leicester Method”, worked. Smallpox death rates plummeted, when comparted to the rest of the UK and elsewhere.6
Smallpox is gone
The eradication of smallpox in the wild is often credited to a global vaccination drive initiated by the World Health Organisation in 1966. While the vaccination drive may well have made a contribution, it should be understood that the programme did not mean that the population of the planet was vaccinated against smallpox. Far from it. Worth noting that the smallpox vaccine deployed by this programme was developed in the modern era and was nothing like the vaccine used in the 19th century. One important factor rarely mentioned now, was a change in strategy adopted by the programme leader, Donald Henderson, who led the campaign from 1967 to 1977. Facing vaccine supply challenges in Nigeria, Henderson decided to change approach, and began to focus on aggresive case-finding, following up with vaccination for nearby persons. This approach, now termed containment vaccination, led to the eradication of smallpox in the region despite vaccination coverage of well less than 50% of the population. Indeed Henderson credited the success of the whole programme, primarily to the “surveillance-containment” strategy7. Interestingly and as an aside, in later life he was to voice criticism of social distancing as a credible pandemic measure. His wisdom on this topic, largely ignored throughout the COVID public health response!8
The belief that smallpox was eradicted in the wild through vaccination often leads to claims that other diseases can be eradicated permanently using vaccination programmes. Such ambitions are almost certainly unattainable, for the simple reason that smallpox is a very unique virus — smallpox has no known animal or non-human reservoirs 9. This means that if the virus is eradicated from all humans, then it no longer exists in the wild, unless re-introduced from laboratory specimens. This contrasts with other viruses (such as polio), which lie dormant in animals and can then jump to humans and infect them. In practical terms this means viruses which exist in animal reservoirs can never be eradicated, and suppression of the viral infections leading to diseases caused by such viruses, requires that vaccination continues ad-infinitum for all humans. Polio, for example is close to being eradicated in the wild. If we were to then stop polio vaccinations for newborn children, eventually the virus would again jump from animals and infect these unvaccinated children.
If you want to learn more about Edward Jenner, then a favourable perspective would be his biography The Life of Edward Jenner (Vol 1 and Vol 2) written by John Baron, published in 1838. While a critical perspective can be found in Charles Creighton’s book Jenner and Vaccination: A Strange Chapter of Medical History, published in 1896.
2. Our immune system
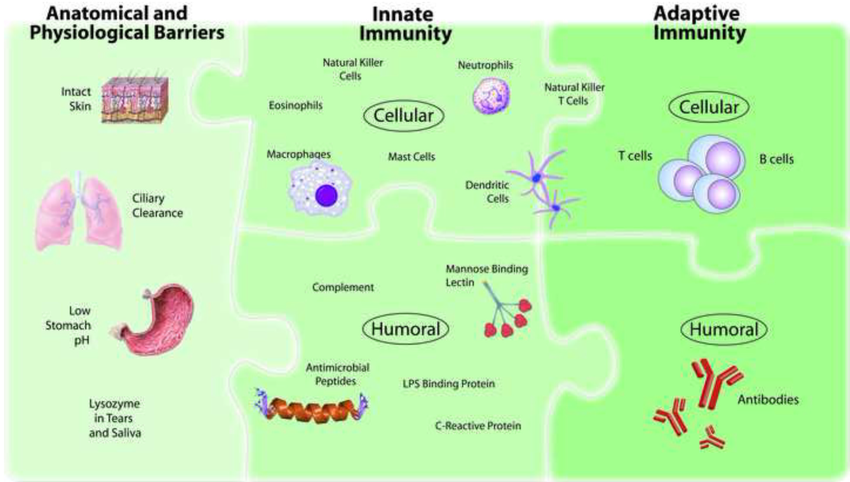
How the human immune system works is a vast topic and not one that I will be able to do full justice to here, not simply because it is vast, but also because there are many facets of immunity and our immune system that remain not well understood. The immune system has three elements: physical and chemical barriers, innate immunity, and adaptive immunity. These are shown in figure 1 below.
Far and away the best resources I have found to explain all of the many component parts of our immune system are this article on the geekymedics.com website, and this website.
When the body is exposed to a pathogen, our immune system (hopefully) kicks into action, neutralising or killing the pathogen thereby preventing illness, and also training our immune system to protect us from future infection by the same pathogen.
As mentioned above, our immune system has different component parts, and these parts come into battle as layers. In Figure 1 above, the order of coming into battle flows from left to right. Our skin layer could for example repel some pathogens and prevent inflections. Next, the innate immune system will get called into action to battle any pathogens that breach the physical/chemical barriers. This part of the immune system is non-specific, meaning that it isn’t deploying a defense that is specific to the type of pathogen being fought. It’s a bit like a blindfolded soldier running at the enemy swinging a studded club in all directions. That soldier will likely take out some enemies, but wouldn’t defeat an army. Next, the adaptive immune system gets called up. The adaptive immune system is specific, so it attempts to mount an attack that is tailored for the pathogen being fought. These are our more specialised and well-trained forces, examples being B cells and T cells.
T cells are white blood cells that are involved in acquired immunity and there are three types: helper, killer (cytotoxic), and regulatory. Helper T cells oversee cytokine signaling to activate B cells and increase the efficiency of other immune cells, such as macrophages. Cytotoxic T cells are important in viral infections in that they kill cells that have been infected by viruses. Regulatory T cells regulate the immune response. They signal for increased activity early in an infection, and conversely, signal for a decrease in the response as the infection is brought under control.
B cells are also white blood cells, which produce antibodies specific to the antigen that stimulated their production. Antibodies secreted by B cells are a crucial weapon of the adaptive immune response. They are specific for the pathogen that is attacking, so they can bind to and neutralise it. There are five different types of antibodies that the immune system can generate:10
- IgM – this has a pentameric structure. It is expressed on B cell surfaces and produced early in the immune response whilst IgG is being generated.
- IgG – this has a monomeric structure and provides the majority of antibody-based immunity. It is found mainly in circulating blood and tissues (it also crosses the placenta to provide passive immunity to the fetus).
- IgA – this forms a dimeric structure once it reaches its target tissues. It is found in mucosal areas such as the GI, respiratory and urinary tracts. It is also secreted in saliva, tears and breast milk.
- IgE – this has a monomeric structure. It binds to allergens and mediates allergic reactions, as well as providing immunity against multicellular organisms such as parasitic worms.
- IgD – this has a monomeric structure and is rather mysterious. It is found in very low levels in the serum, and appears to interact with basophils and mast cells.
These adaptive parts of the immune system might not all be needed. Perhaps some IgG antibodies are enough to defeat the enemy. If not, more and more forces are called into action. Most of the cells that are activated during an infection die during or shortly afterward. However, a small subset of both B and T cells can remain indefinitely. They are called memory cells. These memory cells recognise specific antigens. For example, most of us have memory B and T cells that monitor our body for influenza. Whether our first encounter with influenza was an infection or the result of vaccination, our immune system went through the process of becoming activated and responding to the assault. This first response is called the primary immune response. The memory cells that remain after a primary infection serve as guards watching for influenza to appear again. If it does, these cells will quickly activate allowing the immune system to produce a faster and more efficient immune response to this second (or third or fourth, etc.) attack.11 This means that our immune system does not need to be constantly pumping out billions of antibodies to protect against each of the many thousand pathogens that might cause illness. When the pathogen arrives, the immune system can react, producing the appropriate antibodies and defences against that pathogen.
The extent to which the immune system armed forces are called into action can depend on the nature of the pathogen, how it turns up, and also, in the case of viral infections, the viral load (how big is the enemy army). A low viral load might well be seen off by very early layers of your immune system, and if this was the case, then you would not even have bothered to enlist the services of B and T cells, or developed memory cells to protect against future attacks. The same could be true if the pathogen is not particularly dangerous. A respiratory virus in your upper respiratory tract would typically trigger fewer immune response elements than were it to reach your lungs. This is partly because some generalist forces like macrophages are prestationed there in the upper tract, and attack the pathogens as they enter. That is why most colds and flus never even make it to the lungs. This all makes natural sense. Our immune system resources are not infinite. There is no point calling up the full army to deal with a single enemy who is carrying a catapult and stone. It is a costly endeavour to train up those specialist T and B cells, so best to save that effort until an enemy that warrants deploying them, turns up.
As a general rule of thumb, the broader the immune response, the longer lasting the immunity memory will prove to be. Antibodies fade away quickly. Memory B and T cells can persist for a lifetime. This is an important point: antibodies fade away quickly.
3. Viruses 101
Some basics now about viruses and about SARS-CoV-2.
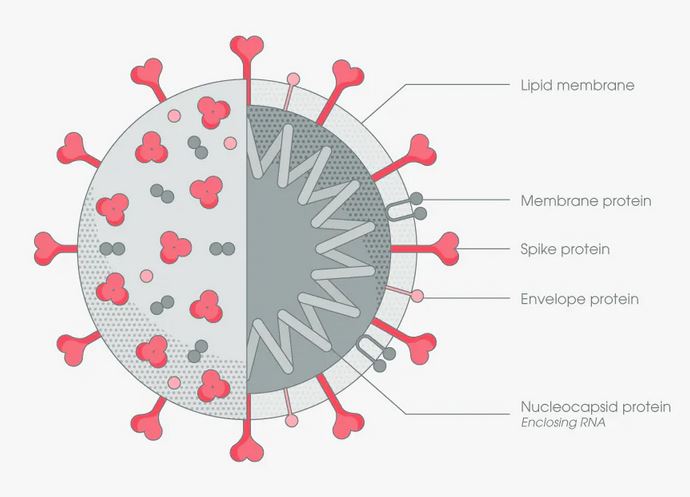
SARS-CoV-2 is a virus, COVID-19 is a disease, caused by the SARS-CoV-2 virus. Figure 2 below shows the structure of the virus.
You will probably be familiar with the general principle of how viruses work. Viruses want to be top in the popularity polls. Their ambition is to spread. “Copy me and pass me on” they say. This being the case, killing their host is not a great way of achieving that ambition. As such, viruses mutate and evolve, and the natural evolutionary path of these mutations is to cause the virus to become less virulent (deadly) and more transmissable. The way in which a virus goes about “making copies” of itself, is that it hijacks the DNA of a cell in your body to make those copies. To do that, the virus needs to gain access to the cell through the protein wall of the cell.
Not all viruses behave in the same way though, and their access strategy through the cell wall vary. The measles virus for example, uses a really complicated strategy which requires specialised proteins on its surface to create a doorway through the wall. That complex strategy leaves little room for error in the subsequent copying process. If the copying process creates a slight variant, then that copy won’t have an access strategy that works, and thus that slight variant virus can’t get in to a cell to copy itself and so that mutation meets an evolutionary dead end. So with measles, even with loads of mutations going on, those mutations are usually all evolutionary dead-ends, and so the measles virus is said to have low genetic drift, in other words, genetic variants that survive rarely if ever happen. And this is why with measles, infection or vaccination gives a lifetime of protection — new variants don’t change much over time. Polio and smallpox also have very low genetic drift for the same reason.
A virus like influenza on the other hand, is different. Influenza viruses have a very simple and uncomplicated cell access strategy — they lock onto one of the sugars on the outside of the human cell, and when the human cell pulls the sugar inside as a source of energy, the virus piggybacks that journey. This is so simple, that this allows the influenza virus to go through lots of mutations without losing its cell entry capability.
Most RNA respiratory viruses adopt simple cell entry strategies and thus have high genetic drift: lots of variants emerge and persist. Coronaviruses use a different entry strategy to influenza viruses. Coronaviruses use the (now famous) S-spike protein on their surface, to latch onto a receptor (ACE2) on the target cell, which acts as a kind of key to unlock a door on the cell wall. This is more complicated than the influenza method, but still relatively simple, and so coronaviruses also have high genetic drift.
We come on to vaccines in the next section, but this helps explains why influenza (flu) jabs are fairly rubbish. For any fast-mutating viruses like influenza or coronaviruses, any immunity you have, either from infection or a jab, only offers protection for a limited time, after which there are sufficiently different variants floating around to give you a new infection from a different but closely related cousin of the variants seen previously. You only ever get some partial protection from infection/jab, towards the next infection by a new variant. You’re never 100% protected against the next variant, but neither are you 0% protected. There is always enough carry-over to give some protection, and this is called cross-reactive immunity.
So to summsarise, some viruses have complex cell entry techniques, and thus see very few variants emerge due to low genetic drift. Others have more simple cell entry strategies, and consequently more frequent variants emerge due to the high genetic drift. Most of the content for this section came from “Autopsy of a Pandemic”, by Julius Ruechel (2021).
4. Vaccines 101
Today, we have vaccines for various diseases. Vaccines are made using several different processes. They may contain live viruses that have been attenuated (weakened or altered so as not to cause illness); inactivated or killed organisms or viruses; inactivated toxins (for bacterial diseases where toxins generated by the bacteria, and not the bacteria themselves, cause illness); or merely segments of the pathogen (this includes both subunit and conjugate vaccines). Vaccines using these various mechanisms are deployed against measles, mumps, rubella (MMR combined vaccine), Varicella (chickenpox), Influenza (nasal spray), Rotavirus, Polio (IPV), Hepatitis A, Diphtheria, tetanus, Hepatitis B, Influenza (injection), Haemophilus influenza type b (Hib), Pertussis, Pneumococcal, and Meningococcal.12 This table gives a good summary of which vaccine mechanisms are deployed against which pathogens.
The immune reaction to a pathogen introduced through natural infection, outlined above in section 2, can also be induced through vaccination using the methods described above. When vaccination causes our immune system to train against future infection, this is often referred to as conferring sterlising immunity. The concept of sterlising immunity is a hotly debated topic, and indeed even the defintion and very existence of sterlising immunity is not settled or agreed. Does it mean that a pathogen cannot ever again infect a person at all? What if a virus manages one single cell replication and is then killed? Or how about an infection with a viral load which never achieves sufficient magnitude to cause disease or transmit infection? All, and more, could be reasonable definitions.
Regardless this debate, the layman understanding of most if not all traditional vaccines is that once taken, they mean that infection and illness are prevented and pathogen transmission is prevented, in a practical and real-life sense. In the case of a virus for example, once vaccinated, the virus cannot use you as a transmission vector.
We can refer to vaccine definitions, commensurate with this understanding.
Vaccines which successfully confer sterilising immunity are often referred to as “perfect” vaccines, examples of which are many of the well-known common childhood vaccines like the measles vaccine. Vaccines which do not confer sterilising immunity are often referred to as “leaky” vaccines13. Many (all?) influenza “shots” for example are “leaky”. This illuminated something important that I have previously paid little or no attention to, or was even aware of. In most of my lifetime, it now seems to me that the concept/phrase ‘vaccination’ has been applied to both vaccines that are perfect, and vaccines that are leaky. But the consequence of this is that it skewers the universal belief that getting a vaccine prevents infection — for example, leaky flu vaccines can’t and don’t prevent infection. So a much more accurate view of things would be that we’ve been using some perfect vaccines like the measles vaccines, which prevent infection and therefore fully protect against disease, while also using some leaky vaccines like the flu shots, which might prevent infection against some flu variants but not others, and might help reduce the symptoms of the disease should infection occur. Perhaps this is why flu “vaccines” are often referred to as flu shots or flu jabs, as this avoids the word vaccine and with it, any (incorrectly assumed) suggestion that infection is prevented. I will come back to this later.
A long and detailed article all about vaccines can by found at The Nature journal, here. And a comprehensive website about vaccines, can be found here.
5. What do the COVID jabs do (and not do)?
Now we can finaly turn to the COVID jabs. The Pfizer jab uses mRNA technology while the AstraZeneca jab uses an adenovirus vector, both technologies being very new in the world of vaccine development. For the mRNA jab the genetic instructions for how to make the spike protein are encoded onto a messenger RNA strand. That mRNA strand is then enclosed in a lipid nanoparticle to protect it. These are then injected into the upper arm. The lipid cells fuse with human cells and the mRNA spike protein-building instructions go to the part of the human cell where proteins are manufactured. The spike protein is then manufactured by the human cell and the spike appears on the cell surface. The different COVID jabs currently in use, each include encoded building instructions for the SARS-CoV-2 spike protein, either completely or partially, and potentially also with some additional modifications/adaptations.14 15 For viral vector vaccines, genetic material from the COVID-19 virus is placed in a modified version of a different virus (viral vector). When the viral vector gets into your cells, it delivers genetic material from the COVID-19 virus that gives your cells instructions to make copies of the S protein, which once again then display on the surface of the human cell.
Upon seeing this spike protein, the immune system of the jabbed individual then produces antibodies which attack this modified spike protein, and the individual likely develops memory B and T cells, tuned to attack against the modified spike protein. Should the individual then subsequently actually meet the virus, the body’s immune system (hopefully) responds to the presence of the spike protein of the virus because that spike is sufficiently recognisable against the modified spike protein that was previously seen in the jab, and for which antibodies and memory B and T cells have hopefully been developed for.
The immune response from the COVID jabs is thus a different response to that which occurs through natural infection. The jab immune response is a response to the spike protein (in its modified form) alone. The immune response to infection is a response to the whole virus, not just the spike protein (or a part of it). For some considerable time during 2021, there was a bit of a battle going on within the scientific community about which was superior: the jab-induced immune response alone, immune response driven by infection alone, or immune response from a jab following an infection, or infection following a jab. This battle appears to have reached a conclusion with quite a number of studies16 17 18concluding that protection through natural immunity developed from infection is broader and more persistent over time than that offered by the jabs, or infection followed by jab (sometimes called hybrid protection).
What some commentators almost certainly did during this debate intentionally or unintentionally, was conflate two different things. The jab induces a narrower immmune response than natural infection. The jab does also, however, induce production of very high quantities of IgG antibodies to the modified spike protein. This second point is harnessed to then make statements like “top up your immunity by getting jabbed…the jabs give you a huge level of immunity/protection”.19
“There’s a very clear message out there that ‘OK, well natural infection does cause immunity but it’s still better to get vaccinated,’ and that message is not based on data,”
“There’s something political going on around that.”
Monica Gandhi, infectious disease specialist at University of California, from Vaccinating people who have had covid-19: why doesn’t natural immunity count in the US?, BMJ
What do the jabs not do? Well, they do not prevent infection and they do not prevent viral transmission. This is a very important point for me. If you have read this article up to this point, I suspect you will have noticed that I have not once described the COVID jabs as vaccines. And that is because they are not “perfect” vaccines, because they do not confer sterilising immunity from the virus or disease.
The evidence on infection, and then transmission, is clear. Let’s look at it.
Here are two tables from the UKHSA Vaccine Surveillance Reports, setting out infection levels. The first, Figure 5, covering weeks 35 to 38 in 202120, which is the four week period up to 26 September 2021. The second, Figure 6, covering the 4 week period to 30 Jan 202221.
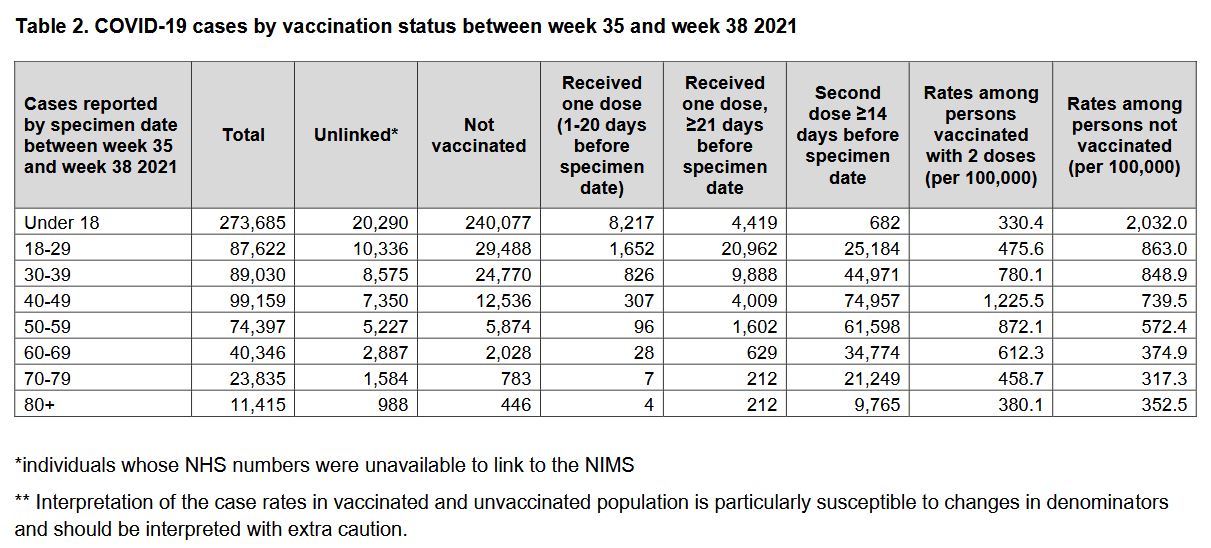
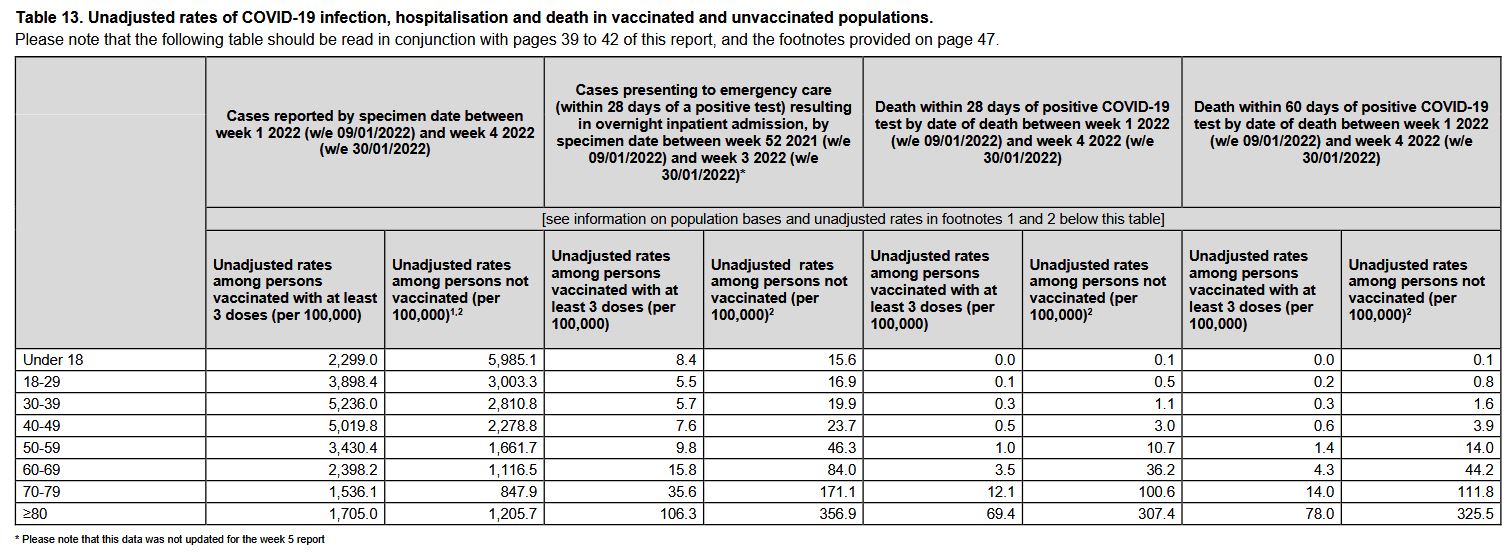
The simple fact that there are data published showing infections in the jabbed shows that the jab does not prevent infection. The table in Figure 5 shows that back in September 2021, every age group 40 and above, had infection levels (per 100,000 population) greater in the jabbed than the unjabbed. From the table in Figure 6 we see that in January 2022, EVERY age group apart from the under 18 group, had infection levels higher in the jabbed than the unjabbed. The UKHSA did not publish this data prior to the period shown in the first table, but this means, without doubt, at least since September 2021, the jabbed get more infected than the unjabbed. So not only does the jab not prevent infection, the jabbed are more prone to infection than the unjabbed.
What about transmission? Both the CDC in the US22 23, and UKHSA in the UK24 conducted studies which found that following infection, onward transmission was happening in equal measure in jabbed persons versus unjabbed persons. So there you have it. The jabs, and the jabbed are making spread WORSE, not better.
“The analysis further suggests that whether an infected individual is themselves fully vaccinated or unvaccinated makes little or no difference to how infectious they are to their household contacts.”
The Guardian, 21 Oct 2021
So these jabs don’t confer sterilising immunity, and ought not to be called vaccines. What are they then? They are drugs. Drugs which evidence shows, help mitigate against the development of serious illness should you become infected by the virus. It has of course become controversial to say “These jabs aren’t vaccines”, but it should not be controverial because it is true — something which was pointed out very eloquently by Dr Peter Doshi, who is Senior Editor at the British Medical Journal, captured in this clip (which is 5:44 long, but worth the watch):
As an aside, not so much in the UK but very much so in the US, in the early days of jab rollout public health officials, members of the government and high-profile media commentators blatantly lied about the fact that the jabs did not prevent infection. Here are three videos showing this, the first is Rochelle Wolensky, Director of the Centre for Disease Control (“CDC”) in the US, the second is Rachel Maddow of MSNBC and the third, President Joe Biden.
6. Making vaccines is difficult…
Vaccinologists and immunologists will be very aware of three watch-outs when designing and developing vaccines. These are “leaky” vaccines, Antibody Dependency Enhancement, and Original Antigenic Sin.
Leaky vaccines
I have already mentioned a little about the evolutionary path of a virus, which ordinarily drives the virus to be more contagious and less deadly. The virus relies on its host to spread, so an active, mobile, lively host is more useful that a bedridden or dead host. This ‘evolutionary pressure’ to mutate can be a bit hard to grasp. How could a virus possibly look around, see which mutations are becoming more “successful” and make choices to mutate itself in that direction in order to move closer to virus nirvana of high transmission? The answer is it doesn’t. What is actually happening is that the mutations are random. The virus is applying no intelligence whatsoever. It is the environmental conditions the mutation is born into, together with the capabilities of the mutation (developed randomly), that determines whether the mutation survives/thrives, or is instead eliminated.
Worth noting here, how lockdowns might affect this. Lockdowns meant that, instead of just the ill being bedridden, and the vulnerable shielded, in addition we stopped healthy, active people from circulating. The effect of this is that the mutations produced by the healthy instead of getting maximum chance to spread, get about the same chance to spread as mutations in the ill and shielded. Mutations in the healthy are by definition going to be the less dangerous since they didn’t make their hosts sick enough to confine them to bed. That is precisely the mutation you would like to spread, to drown out competition from more deadly variants. By locking down, this equalises the spread potential of the two cohorts, the healthy with less deadly variants and the ill with more deadly variants. This has therefore artificially created an environment that bucks the evolutionary trend and could cause more deadly variants to win the competition and spread more, thus taking down more healthy people than would otherwise have been the case, and setting up a reinforcing spiral towards more deadly strains.25
This is something we know all about, having observed the events of the Spanish Flu in 1918. With that pandemic, the first wave was not that deadly — like a regular seasonal flu. The second wave was much more deadly, and also hammered young people much harder. What was going on? This is not the evolutionary path that you would predict. The answer lies is the very particular conditions of warfare at the end of WWI — lots of young men trapped in cold, damp trenches. They were locked down! The trenches created an environment that erased the competitive advantage of a mutation that doesn’t immobilise its host, and thus drove the emergence of more deadly strains. When the war ended, the troops left the lockdown-esque trenches, shifting the competitive advantage back to the less dangerous strains, and the flu virus faded away into the background of the regular cold and flu season.26
What problems might a leaky vaccine cause? Consider what is happening. We have a jab that to some degree, perhaps a high degree, lessens potential for hospitalisation or death, but still allows the virus to spread. From an evolutionary perspective this could be very dangerous — a set of conditions where a strain that is very dangerous to the unjabbed, can spread easily among the jabbed without making them particularly ill. This strain has a competitive advantage as it can easily spread in the jabbed. That is bad news for the unjabbed, but also for anyone jabbed but where the jab effect has faded over time. This would create a world where boosters are needed permanently.27 More on this topic here if you are interested: “Imperfect Vaccination Can Enhance the Transmission of Highly Virulent Pathogens“.
Hang on a minute, you say. What about the flu jabs? They are leaky, but they don’t create more dangerous strains. There are several reasons for this. First, flu jab rates only ever get to around 35-45% of populations. So more dangerous strains will face competition from less dangerous strains circulating in the large unjabbed group. Second, the flu jab is only around 40% effective from the outset, and it fades quickly. This means it is less likely to see a more dangerous strain emerge in the jabbed group. That all said, if flu jabs were pushed to be extended to everyone, that might change things, for the worse.
All of this ‘theory’, came to pass in the real world, with a universal leaky herpes vaccine given to chickens since 1970. That vaccine proved to be lethal for unvaccinated chickens, pushing a viral mutation that killed 80% of the unvaccinated.28 As a consequence, we now have a situation where chickens must have a constant stream of vaccinations against the virus.29 30
So to summarise, a leaky vaccine is one which attempts to reduce the impact of symptoms once infection occurs, but it does not achieve sterilising immunity — it allows the virus to infect, and for the infected to then spread the virus. The issues outlined above might never come to pass with the COVID jabs, but striving for massively high vaccination rates is exactly what will create the ideal conditions for this. A leaky vaccine used sparingly to target the more vunerable is a very different thing to one applied to everyone.
Antibody Dependency Enhancement
Immune responses to pathogens involve many cells and proteins of the immune system. Early during an infection, these responses are non-specific, meaning that although they are directed at the pathogen, they are not specific to it. This is called innate immunity. Within a few days, adaptive immunity takes over; this immunity is specific to the invading pathogen. Adaptive immune responses include antibodies. A major goal of antibodies is to bind to the pathogen and prevent it from infecting, or entering, a cell. Antibodies that prevent entry into cells are called neutralising antibodies. Many vaccines work by inducing neutralising antibodies. However, not all antibody responses are created equal. Sometimes antibodies do not prevent cell entry and, on rare occasions, they may actually increase the ability of a virus to enter cells and cause a worsening of disease through a mechanism called antibody-dependent enhancement (“ADE”).
ADE occurs when the antibodies generated during an immune response recognise and bind to a pathogen, but not only are they unable to prevent infection, Instead these antibodies act as a “Trojan horse,” allowing the pathogen to get into cells and exacerbate the immune response and accelerate infection rather than prevent it.31
ADE is quite common within vaccine development, for example with vaccines for RSV, Dengue Fever, and coronaviruses(!). This is one of the reasons why vaccines for SARS kept failing — ADE kept happening in animals during early trials. ADE doesn’t happen straight away — it emerges gradually as new variants appear. What tends to happen though, is that ADE events are spotted during stage 1 & 2 trials, and the vaccine trial is then terminated and the vaccine designers go back to the drawing board. Of course traditionally, phase 1 and 2 trials took place over years, unlike those for the COVID jabs which completed in about 4 months.
One final thing to point out about ADE, and about leaky vaccines. The issues these factors cause — deaths, worse infections, get triggered by variants. And then the vaccine manufacturer pops up with a “new” vaccine to address this “terrible problem caused by the variant”. This might appear to be the vaccine manufacturers riding to the rescue, but that would be a grave misunderstanding. The deaths and worse infections were driven by a badly designed vaccine, not the variants. Variants will always happen in a high genetic drift virus. And that’s a GOOD thing — nature’s way of reducing virulence.
This also offers a useful insight into another reason that deploying leaky vaccines is not clever. Spanish flu is still around today — it is one of the many cold and flu viruses that come and go every year. Sometimes we catch them, sometimes we don’t. If you are immunocompromised or elderly, catching these viruses can be more serious. But each subsequent exposure, teaches our immune system how to keep up with all the gradual mutations that bring new variants. This is the cross-reactive immunity, mentioned earlier in the article. A bit like the regular updates made to the antivirus software on a computer. If it is a mild infection, you might not even notice, but you still get an immune “update”. And when the infection is mild, we know that the immune response will not be so deep, and it will fade with time.32
We also have experience of how less mild coronavirus infections can bring longer-lasting immunity. Consider what the SARS oubreak in 2003 taught us. It was more deadly (11% fatality rate) than COVID, and the antibodies for the SARS virus persisted for >2 years. This is consistent with an understanding that something with a more serious disease triggers a broader portfolio of immune responses and therefore the immune response memory lasts longer. Same with the 2012 MERS outbreak, the most deadly coronavirus we’ve known, with a 35% fatality rate. This proved to have an immune response memory of >6 years. It was clear from very early on, like February 2020, that COVID was nothing like as severe. A case fatality rate of about 1%, they were estimating back then, and even that proved to be an gross overestimate. And thus it follows that immune protection for COVID, whether from infection or jabs, would never be long-lasting.33
In the context of COVID then, this natural method of refreshing the immune system with regular antivirus-like updates, was twisted into hysteria and panic. We rolled out mass testing, and coached everyone who tested positive but was asymptomatic (=healthy), to potentially be frightened and scared of this unharmful immune “update”. Strange.
Original Antigenic Sin
The third and final challenge that vaccine development can encounter is Original Antigenic Sin (“OAS”). Sounds more like some kind of grievous offence in a religious cult. Actually, it is much more serious.
OAS happens when your immune system gets stuck or fixated on offering the immune response which you developed to your first exposure to a virus. Thus when a variant comes along, your immune system starts pumping the immune response developed to the strain you previously saw and got infected by, and developed immunity to. But those antibodies do little or nothing against the new strain. And that is double bad — you are not only spamming the new strain with antibody blanks, but your immune system is 100% thinking it’s doing a splendid job and is therefore devotes zero resources towards combating the new strain.
Clearly then, OAS is highly undesirable. The impact of OAS, particularly in relation to influenza pandemics, is covered very clearly here in a paper from 1960. More recently OAS has reared its head in dengue fever, covered in this paper from 2010 which reaches some frightening conclusions, namely that further vaccination efforts fail to shift the OAS phenomenon, and that the immune system may well be permanently impaired in the fight against future variants.
7. Exploring some data, busting some myths
Before I look at some specific insights from various data sources, a short summary of the key points so far:
- Normal viral evolution sees variants emerge which are more transmissible and less deadly;
- Vaccines which are “perfect”, provide sterlising immunity, preventing infection of, and spread by, the vaccinee;
- Vaccines which are “leaky”, do not prevent infection of, or spread by, the vaccinee;
- For SARS-CoV-2, the jabbed are more prone to infection, and if infected, spread the virus just the same as the unjabbed, and;
- Immunity developed through recovery from infection is broader and more long-lasting than that from the jabs.
Exploring some data
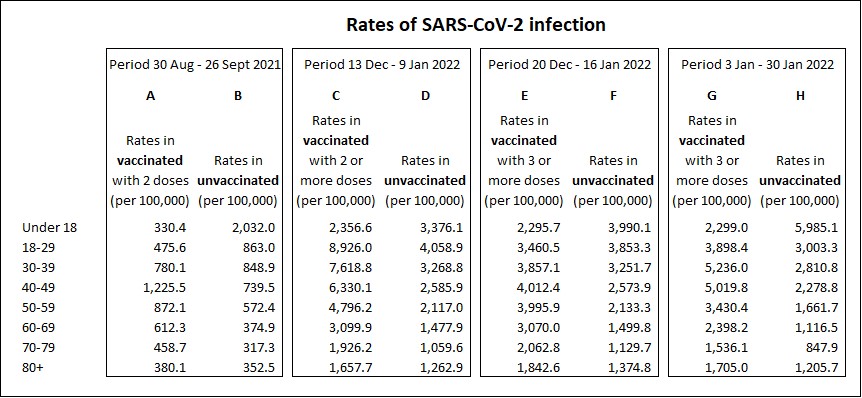
Now let’s examine some data. I have constructed the table in Figure 7 below, from four of the weekly UKHSA Vaccine Surveillance Reports. Columns A & B are jabbed and unjabbed infection rates per 100,000 for the period 30 Aug – 26 Sept 2021. Columns C to H are jabbed/unjabbed infection rates for three other periods, dates as shown in the table.
There is a lot going on in this data, and many insights.
Insight 1
Looking at columns A and B, this is showing us something I have mentioned previously. In all groups over 40, the jabbed are more prone to infection.
Insight 2
Compare columns B and D. These are the unjabbed rates in the September period versus the period starting 13 Dec 2021. For all age groups the infection rates have increased in the unjabbed, and those increases are between 3.3 and 4.7 fold for all ages above 18. What’s all that about then? That, is Omicron, and it tells us that Omicron is much more transmissible. Column B in September was when Delta variant was >95% prevalent, while column D was Dec 21/Jan 22 which was when Omicron was >90% prevalent. From what we covered above, this is good news — Omicron is more transmissible, less deadly!
Insight 3
Now compare A and C. The same idea as from insight 2, but this time we are looking at how the rates changed for the jabbed. WOW. Well, the rates have increased between Sept and Dec/Jan, like they did for unjabbed. But for the jabbed they have increased by anywhere between 4.2 times (the 70-79 group) and a whopping 18.8 times (the 18-29 group). In every single age group, the jabbed are showing even more prone to infection than the unjabbed in Dec 21/Jan 22, than in September 2021. That further increase in susceptibility then sustains at that level, right up to the latest data available.
This explains things like:

Very interesting to read the replies to Victoria’s tweet.
Insight 4
Not so much an insight as a highlight of something potentially suspicious. In column C this is showing the jabbed rate as being the rate for those with 2 jabs. Starting from the following period and onwards, the reports show the jabbed rate as being for those with 3 or more jabs. So that change in data presented, happened just after the week that saw the highest ever rate of infection per 100,000 in th UK since COVID began — a rate of 8,926 per 100,000 in the 18-29 group jabbed with 2 jabs. What happened to the infection rate for the double jabbed in the subsequent periods?? One would suspect that it was even higher than 8,926. I would hypothesise that the boosters are proving totally ineffective at reducing infection risk, with infection risk in triple jabbed still way worse than in the unjabbed. And for those who are double jabbed and not boosted, their situation is even worse than the boosted and deteriorating further as time progresses, with regard to infection risk.
And one other area of suspicion. No data is ever published showing infection rates per 100,000 for the single jabbed. Again, why? They have the data — be complete and transparent, and publish it.
The revelations from insights 3 and 4 really does present quite a shocking situation. For a couple of reasons. First, people are being encouraged to “Get Boosted” when this data shows that a third jab continues to leave you more susceptible to infection — more than even before. Second, and more worryingly, what are the jabs doing that is making it harder for the immune system of the jabbed to resist infection? Let’s think about that, have we touched on anything earlier in this article that might shed light on this? Yes we have — ADE and OAS. Of the two, it looks very much like OAS (although the two are not mutually exclusive so it could be both!) It’s not like these concerns are not real. Pfizer themselves highlighted the concern they had about the ADE risk and their COVID jab.34
A number of studies are starting to appear, testing the hypothesis that OAS is happening. If it transpires that this is what is going on, then the long term consequences for those jabbed could be massive, and not in a positive way.
Busting some myths
Almost certainly the most pervasive myth propogated in the UK in respect of COVID is that the NHS is regularly on the brink of collapse as a consequence of having to deal with COVID patients. And related to this, more recently, the assertion that actually it is unjabbed patients who are responsible for this. “How dare these selfish pricks behave like this – just get jabbed you idiots” would be a common opinion thrown towards the unjabbed.
So is this true? Is the NHS overwhelmed? Is it due to COVID? Are the unjabbed responsible for it all? Let me take these questions one by one. Is the NHS busy?

Well if you turned up in say December 2021 or January 2022, I dare say ICU could have been rammed at that point. It gets like that every year (see Figure 8 alongside). More than 70 Winters have been and gone since the NHS was founded in 1948. You would think by now they could have figured out how not to be surprised that things get a bit tricky during the Winter months?
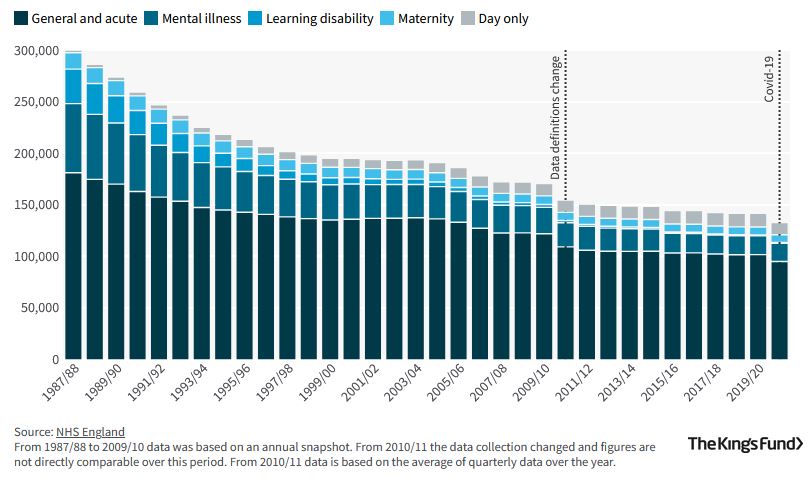
Of course they don’t help themselves. General and acute bed levels have been cut continuously during the past 30 years, as you can see from Figure 9 below.
In England, we have 98,000 “general & acute” beds capacity in our hospitals, and roughly 4,300 critical care beds. During December 2021, occupancy of general & acute beds was running at between 72,000 and 82,000 on any given day.35 For critical care beds in England during December 2021, occupancy by COVID-positive patients was at its lowest on 25 December at 800 and highest on 31 December at 996 while for non-COVID patients the lowest occupancy was 2,122 and the highest 3,763. On no day in December 2021 were the COVID-positive patients in ICU greater than 30% of all patients in ICU.36 Don’t forget that COVID occupancy is not “all people who are in hospital because of COVID”. It means people who are in hospital and who tested positive for SARS-CoV-2 within 28 days of admission. So that covers anyone who had a heart attack, stroke, fell down the stairs and broke their legs, flew through a car windscreen, were shot, stabbed, poisoned, or were suffering from one or more of many other acute injuries or chronic ailments, and also happened to test positive for COVID at some point in the recent past or after they had been admitted. The published data gives no details of the nature and severity of the illnesses requiring critical care for COVID-positive patients. Finally on this topic, during December 2021 roughly speaking, there were as many critical care beds completely unoccupied as there were occupied with COVID-positive patients.
OK, so before we get to whether the unjabbed are a problem, it seems that COVID full stop is not overwhelming ICUs, when less than 30% are there and positive with COVID, nevermind the unjabbed. Nevertheless, what about these unjabbed clowns then? Is it true that everyone in ICU who tested positive for COVID is there because they have caught COVID and are not jabbed?
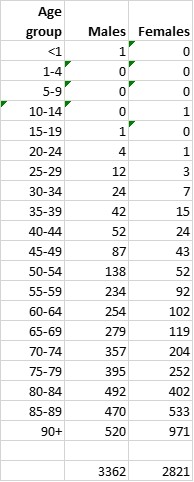
Let’s see what the data says. See Figure 10, taken from the UKHSA Vaccine Surveillance Report Week 51 (covering weeks 47 to 50, 2021).
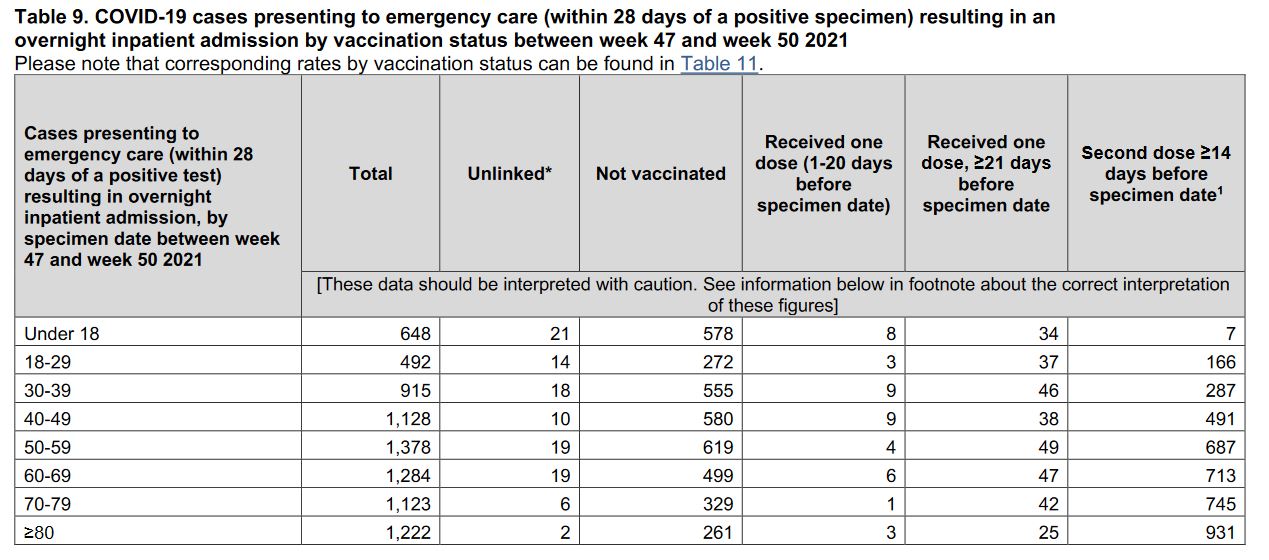
We add up the ‘total’ column and subtract the ‘unlinked’ column to get the total where jab status is known (8,081). Then add up unjabbed, 3,393. Subtract the two and that gives jabbed of 4,388. So 54% jabbed, 46% not.
Yeah but I know what you’ve done there. You’ve done that data fishing thing, where you look at all the data, but only show me the bits that support your argument.
Well, no. How about we look at, say, week 39 here. Unjabbed 2,922. Jabbed, 4,734. Which is 61% jabbed 39% not jabbed. You will need to go way back to say March 2021 when the jab campaign was only getting going, to find a time period when their were more unjabbed in ICU than jabbed. And of course go back far enough, and everyone in ICU was unjabbed, because nobody had been jabbed.
Turning back to the question, which implied that the unjabbed are overloading, bedblocking and generally screwing the health service and putting at risk all those selfless people who got jabbed because “that’s the right thing to do, for the greater good, you know?” Complete rubbish. The unjabbed are a fraction of a fraction of a fraction of NHS general and acute care volumes, and make up about 11% of those being treated in ICU. How do I get to that? Use the numbers from above. In England in December, an average of about 900 ICU beds occupied by COVID-positives and an average of about 3,000 by non-COVID people. In that period 46% of COVID ICU admissions are unjabbed. (900 * 0.46) / (3000 + 900) = 10.6%. So in December 2021 we have 11% of ICU being unjabbed, while at that point there are 19% of the adult England population unjabbed.
You’re shocked. I know. And I’m not surprised you’re shocked, I mean Sajid Javid, Boris, lots of GPs and hospital consultants have been screaming that 90% of people in ICU right now are unjabbed – “So get jabbed, you idiots”. In fact that is what Tony Blair said, literally, as you can hear in the video below.
“We need to target the unvaccinated. Frankly if you’re not vaccinated at the moment and you’re eligible and you’ve got no health reasons for not being vaccinated, you’re not just irresponsible. I mean, you’re an idiot.”
Then we have the NHS consultants thowing around claims that “80-90% in ICU are unjabbed”, like Rupert here, and then ‘helpfully’ tweeted and retweeted by Fergus and Piers:
You will have to ask all of those people why their assertions are not supported by the NHS and UKHSA data. I have no answers for you about that.
Well now, clearly getting jabbed doesn’t mean you have eliminated your potential need for medical care, as the data above shows. But do the unjabbed disproportionately create some kind of burden? Looking at the data again from the UKHSA Vaccine Surveillance Report, it seems clear that the unjabbed DO place more of a burden on ICU. See Figure 11 from the week 51 report of 2021.
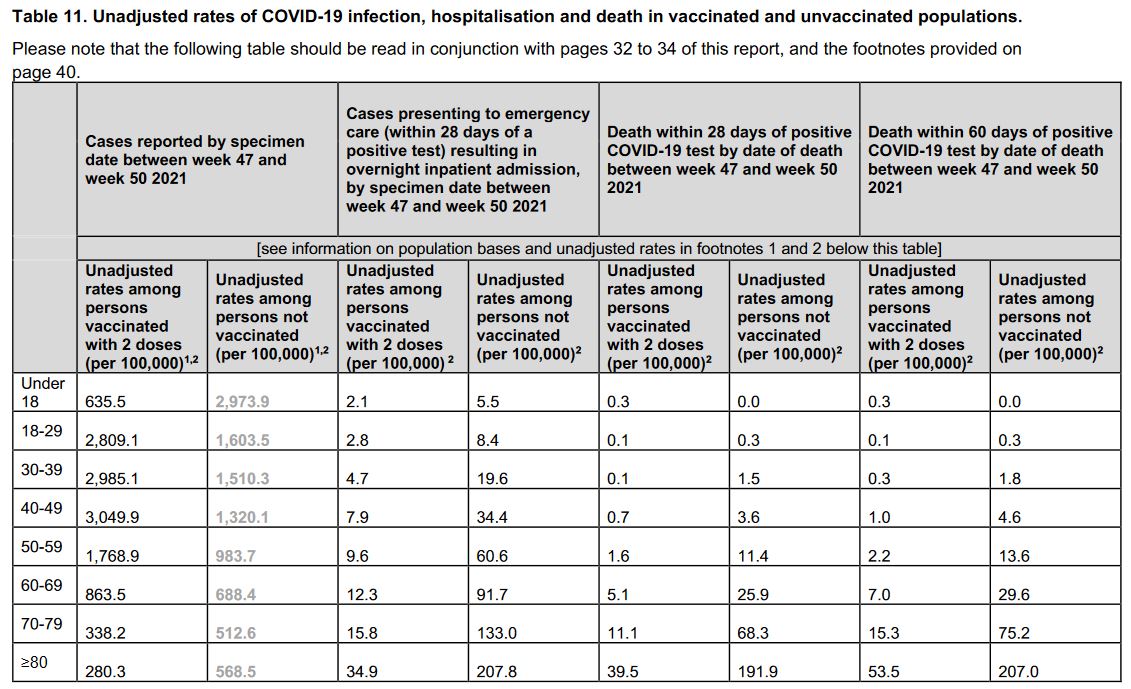
This shows that for every age stratification, unjabbed present at ICU at substantially higher rates than the jabbed. Up to 9 times more often, for example, in the 70-79 age range. Now, in absolute numbers, that means out of a population of about 250,000 people who are unjabbed and aged 70-79, 329 ended up in ICU in the relevant 4 week period that this report is focussed on. Are there likely to be a lot of 70-79 year olds who are quite ill, and in fact with illnesses that mean they are advised not to be jabbed? I would say that is definitely a factor. Of course this argument is not credible in the age ranges below 50, so here, it is reasonable to say that the unjabbed present a disproportionate burden.
There is however, a problem. And it has only really been a problem that has manifested at the beginning of 2022. Again we are back to the UKHSA Vaccine Surveillance Reports, this time for week 4 of 2022. And this article which analyses that report. Below in Figure 12, is the data plotted by age group, showing death rates (per 100,000) within 60 days for no jab, double jab and triple+ jab
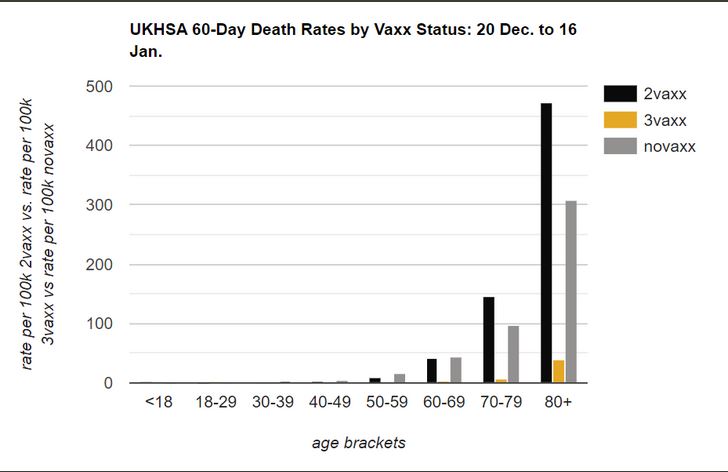
Oh dear. In age group 80+, death rates for double jabbed are nearly 50% higher than unjabbed. Slightly higher for the 70-79 group, and about the same for the 60-69 group. The death rate for the boostered is much lower for all >60 groups.
What in the hell is this telling us? Well, effectively this is suggesting that if you have been double jabbed, you are looking at a higher probability of death than someone who has never been jabbed. It also appears that you can “fix” that problem by getting boostered. However, the booster is the same product that went into your arm for the first two jabs. So it will fade again. So get another booster? And another, and another…
We can also look at Public Health Scotland data, this time figure 13 is showing ICU admissions, by week, by jab status
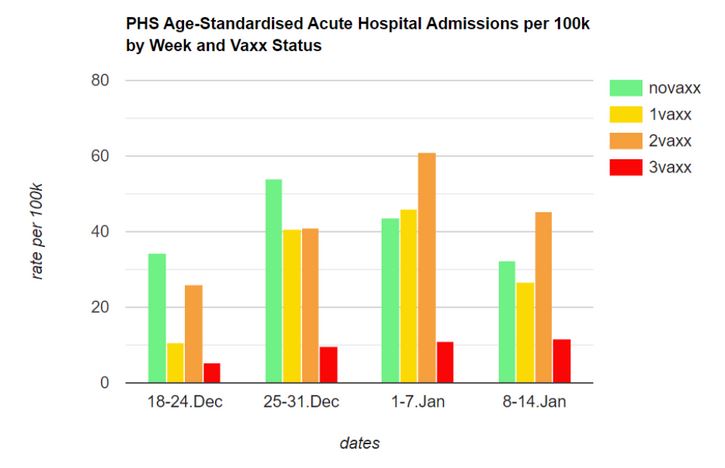
Once again, oh dear. Again these are rates per 100,000. In the week before and the week after Christmas, the unjabbed were most likely to go to ICU. First week of January 2022, and the single and double jabbed were more likely to end up in ICU than the unjabbed. Second week of January 2022, and the double jabbed are again more likely to be in ICU than the unjabbed. This emerging picture for the double jabbed is consistent with the thinking outlined in Insight 4 above.
Now we come back to the original question. Are the unjabbed putting a disproportionate pressure on ICU. The answer is, ‘yes they were’ during the second half of 2021, when jabs dampened the illnesses being driven by the SARS-CoV-2 variants that were circulating at that time, which was primarily the Delta variant, and while during that period the double jabs had been recently administered and therefore still had some effect. Now however, unless you get boosted, the jabbed are a greater burden as compared to the unjabbed. Of course, from now on the UKHSA “data” isn’t going to explain that to you — they’ll still be screaming that one message, “Get Boosted Now!”. And of course, any incremental burden from the unjabbed in that H2 2021 period was still but a small fraction of the workload on ICU.
Just one final point to say on this “burden” thing. Fixating on jab status as the most important determinant of ICU COVID burden, at the expense of any other consideration, would be to miss some really important factors. Can you think of other things that might merit consideration?

Meet Aled. Aled was featured in a story on the news website WalesOnline, a story which got hammered on social media because of the headline caption:
“Young man with clean bill of health left ‘hours from death’
Wales Online, 4 December 2021
in hospital after catching Covid”
“Clean bill of health” is quite a stretch — Aled is obese. Obesity and other comorbidities such as diabetes, are estimated to contribute to between 80 and 95% of COVID hospitalisations37. In the US a study by the CDC determined that 78% of COVID hospital cases were overweight or obese.38 In the UK, the Intensive Care National Audit & Research Centre (ICNARC) reached near identical conclusions, putting the figure at 77%.39 If you’re really worried about pressure on ICU, tackling obesity would be a worthy cause.
By now you might be thinking:
So, I’m right, yes? Everyone should be doing what they are told and getting boostered, then we’ll all be fine. If you don’t do that then that’s your choice, but choices have consequences. You could make a choice that will really help our poor doctors and nurses.
If you are going to say that, then I must insist that you apply your dogma comprehensively and universally. Been smoking 20 a day for the last 30 years sir? What’s that? You’ve got lung cancer and you need treatment? Get out of here — you made a choice, and choices have consequences. We’re not treating you here, selfish prick.
Oh, Aled, it’s you again. What’s that? I’m struggling to hear you, you’re mumbling and slurring your voice. Oh, I see. You’re saying you think you might be slipping into a diabetic coma? Aled, mate, there’s no “think” about it, that’s exactly what’s happening. But you haven’t paid any attention to your health and are clinically obese so you’re not coming in here, selfish prick.
Oh hello, what have we here? You’ve broken both arms and both legs? How on earth did you manage that? You fell while ROCK CLIMBING!? Are? You? Mad? Do you have any idea how risky that is? Well look at you now, serves you right, selfish prick.
And what about you sir, what seems to be the problem? Liver disease? That’ll be the bottle of wine a night for as long as you can remember, that’s what’s done that. But, I’m puzzled, why have you come to us? You want TREATMENT!? You must be joking — get the hell out of here, selfish prick.
Exploring data, busting myths – Summary
To recap on this section:
- With the arrival of Omicron, it appears that the propensity for the jabbed to get infected has accelerated — the jabbed are now much more prone to infection than they were, and way more than the unjabbed;
- Something strange is happening with the immune system of the jabbed — unless you get boostered, your immune system seems to be impaired in the fight against infection;
- The NHS is not any more busy in ICU than any other time in recent history, COVID positive patients make up a small proportion of ICU activity (~24%), and the unjabbed represent about 11% of ICU occupants;
8. My decision to decline the jabs
I have set out here 5 factors labelled A to E (summarised at F) which either initially led me to conclude that I would not get jabbed, or subsequently reinforced my decision not to get jabbed. I have tried for the most part to put them in chronological order.
A. Instinct
I can recall around late Summer or early Autumn of 2020, a conversation with my father-in-law who said “They’re now talking about having COVID vaccines available early next year, and if that happens it will put an end to all this.” My instant reply was “I just don’t believe that. Vaccines take years to develop, and then test. I just can’t see how that will all happen within a year.” At that point I had never heard of mRNA research or mRNA vaccines.
Then, on December 8, 2020, Matt Hancock, Secretary of State for Health in the UK, announces that vaccines are now ready and being rolled out.
On December the 2nd 2020, the Medicines and Healthcare Regulatory Authority (“MHRA”) issued a temporary authorisation for the Pfizer/BioNTech COVID jab. The authorisation was made under Regulation 174 of the Human Medicine Regulations 2012 Act (as amended), which allows for temporary authorisation for an unlicenced medical product in emergency situations. The AstraZeneca COVID Jab was also given temporary authorisation on 30 December 2020.
Retrospectively, I can’t now pinpoint the exact date or time I first decided that I would not get jabbed, but I can say that the first and most significant factor in that decision was pure instinct. I can’t fully explain why, but I sensed there was something wrong, something suspect about the whole thing. The media were in overdrive, waxxing lyrical about this wonderful new type of vaccine technology, and that redemption was just around the corner. Meanwhile I was thinking to myself, why is everyone rushing to get something that is so new in developmental terms. When I say new, I do recognise that mRNA vaccine technology had been in research for more than a decade. But that research had not turned out a single workable vaccine product. What a miracle then, that the first mRNA “vaccine” product that was ‘viable’, just happened to be the one that big pharma churned out for COVID. What are the chances!?
Also worth recalling that in the early months following the beginning of jab rollouts, nobody was even talking about anyone my age needing a jab — this was “15m jabs to freedom”“15m jabs to freedom”, The Daily Mail, 27 December 2020, prioritising the elderly and clinically vulnerable.
B. Rapid trials
The clinical trials for these jabs were undertaken at break-neck speed. Phase 1 and 2 trials were started in April 2020 and finished by July of that year. Phase 3 trials then commenced, while in parallel, medical regulatory authorities across the world handed the jab manufacturers emergency use authorisations. The phase 3 trials will not complete until 2023 at the earliest. For me, this is just bonkers. I was and am not prepared to try something like this that hasn’t been comprehensively tested.
My concerns about the trials, and the results from them, are not allayed when I see the FDA in the US propose to wait 75 years (!) to release the trial and safety data on which they based their decision to grant emergency use authorisation for the Pfizer jab. This ludicrous proposition was set aside by a judge in January 2022, who directed the FDA to release all the documentation within 8 months.
C. My risk profile is tiny
Professor, and now Sir, Chris Whitty said it himself towards the end of April 2020. “For any individual person, the chances of dying from coronavirus are very low.”
Now, 22 months later we have much more real world data, and we can see if Whitty was right. The ONS recently released the data on numbers of deaths where COVID was the only listed factor, and thus no comorbidities were involved. Here it is, by age range, in Figure 15. This data will shock many people. “Nah, that’s just wrong. My tellybox has been telling me that over 150,000 people have been killed by COVID.” Well the data is correct — from Feb 2020 to Dec 2021, it was 6,183 people in the UK killed by COVID only. It means that the other ~144,000 died with COVID and comorbidities.
I’m not going to bother outlining here the staggering number of reasons why even these figures are grossly overstated. That might come at some point in a different article. The main point I need to highlight here, is that I am a fit and healthy 49 year old with no comorbidities. So for people like me, in 22 months, 87 lost their life to COVID. That is tragic for those 87 people and their families, but nevertheless that represents a survival rate greater than 99.9999%. I have more chance of meeting my death by drowning.
D. Adverse effects from the jabs
You have been well and truly saturated by relentless informational campaigns, drilling home the same message, over and over.
“Safe and effective.”
“Safe and effective.”
“Safe and effective.”
“Safe and effective.”
Even a remote suggestion that the jabs might have adverse effects is being stamped on by the government and the public health establishment. They’re even using your money to pay celebrities and influencers to jump onto the bandwagon.
So I can completely understand why people would have the view that these jabs are a no-danger, no-regrets ticket (notwithstanding everything I have outlined about the fact that they don’t actually perform anything like as well as you are being told). But there is substantial evidence mounting that the jabs are causing problems. Let’s explore one particular thread on this. I am a football fan. And the answer to your next question is ‘Arsenal’. If in 2020 you had asked me “When have you seen or heard of football players having heart problems?” I would only have been able to cite three examples.
The first is Marc-Vivien Foé. Marc-Vivien was playing in a FIFA Confederations Cup match in 2003, and collapsed on the pitch. Despite attempts to revive him, he died within hours of collapse. An autopsy revealed a hypertrophic cardiomyopathy, which is a hereditary heart condition.
The second is Fabrice Muamba. Playing for Bolton against Spurs in March 2012, Fabrice suffered a heart attack while on the pitch. He received treatment on-field, including numerous defibrillator shocks and though his heart stopped for 78 minutes, Fabrice recovered.
The third is Nwankwo Kanu. Kanu was signed by Arsene Wenger in 1999 with full knowledge that Kanu had a congenital heart defect present since birth and operated on in 1996, when it was discovered. I was a big fan of Kanu, and his success on the pitch certainly showed that he wasn’t encumbered by his condition. His finest day in an Arsenal shirt was the game on the 23rd of October 1999 against Chelsea at Stamford Bridge. 2-0 down after 75 minutes, Kanu proceeded to score a hat-trick within the final 15 minutes to secure a 3-2 win for the Gunners, the hat-trick secured with this worldie in the 90th minute.
So three instances I can recall in 45 years of my life of watching football up to 2020. So what about 2021? This article in the Berliner Zeitung lists 24 instances of player or staff collapses at or during football matches in the past year, and it really only covers instances from a handful of countries, in a five month period. While this article includes a long list of instances going back to June 2021. Caveats are needed here. These reports are not medical studies, and not all the instances listed can be confirmed as heart-related, with some simply reporting a player or coach collapsing. It is though, fair to ask “What is going on? And why are these events not being formally investigated? And why so many?”
The reason people are positing the hypothesis that these collapses are jab-related, is that the jabs are now known40 41to be involved in driving myocarditis, which is a serious condition affecting heart muscles, causing inflamation. The myocarditis link has been played down for months, with the public health fraternity claiming it is “very very rare”, however that picture is now changing. For example, see this study which indicates a doubling of myocarditis incidents in April and May of 2021, compared to previous period averages, and this study from Israel42, that estimates instances of myocarditis in young people, driven by jabs, at 1 in every 3,000-6,000 jabbed individuals of those ages. Now there are about 12.5m people in the UK aged between 12 and 24 who have been jabbed43. So that’s between 4,000 an 8,300 kids who have been injured by the jabs and landed with a serious condition for the rest of their life. And remember that table above about deaths from COVID only. For people aged 12-24 in the UK, there have been, wait for it, seven deaths. That is really not an acceptable risk-benefit equation, in any way, shape or form. What about the damage that could be done to kids from COVID, that doesn’t kill them, I hear you say. Ah yes, long COVID, is that what you mean? Well they looked at that – see here. Conclusion: not a thing, for children.
There are also concerns about blood clots and strokes.
Personally, I am most concerned about what the spike protein might be doing to the body. Many articles can be found on the internet saying the spike protein is harmless. So-called fact check organisations have published many statements saying the spike protein is harmless. If that is true, then why does the COVID jab with the spike protein, drive an immune response? Why would the body react, if the spike is harmless?
Introducing the spike protein with an mRNA jab is also vastly different than the spike protein being introduced via infection with the virus. With viral infection, the spike is part of the virus, and SARS-CoV-2 is a respiratory virus and thus seeks to attack the body through the respiratory system. As we have learned above, when that happens, a very natural and broad immune response is triggered to counter the virus, including its spike protein.
When the spike protein is introduced via a jab, this is delivered into the muscle tissue in the upper arm. The mRNA genetic code in the vaccine also delivers the instructions which cause the body to manufacture huge additional quantities of copies of the spike protein. Where do these go? Clusters of the spike protein have been found in the spleen, ovaries, heart, brain, lymph nodes and liver of the jabbed.
So overall, I am far from convinced that the COVID jabs are “Safe”.
E. Trust, or lack of
As time passed by, I gradually lost all trust in the political and public health leadership in the UK on COVID. Here are some of the things that happened that eroded my trust in them.
“Mask are useless, sorry, I mean really important…”
On 3 March 2020 on a Sky News segment, Chris Whitty spoke about wearing masks:
“In terms of wearing a mask our advice is clear, that wearing a mask if you don’t have an infection really reduces the risk almost not at all. So, we do not advise that.”
Chris Whitty, Sky News, 3 March 2020
On 3 April 2020, Jonathan Van Tam made a very clear statement about the use of facemasks by the general population during a pandemic.
“There is no evidence that general wearing of facemasks by the public who are well, affects the spread of the disease in our society.”
Jonathan Van Tam, Downing Street Coronavirus Briefing, 3 April 2020
Van Tam and Whitty were not alone in holding this view. In this video we have Anthony Fauci, Head of the National Institute of Allergies and Infectious Diseases in the US.
“There’s no reason to be walking around with a mask. When you’re in the middle of an outbreak, wearing a mask might make people feel a little bit better and it might even block a droplet, but it’s not providing the perfect protection that people think that it is. And, often, there are unintended consequences — people keep fiddling with the mask and they keep touching their face.”
Anthony Fauci, interviewed on CBS 60 Minutes, 8 March 2020
And here we have a video from the World Health Organisation which was in place until June 2020.
From June 2020 onwards, suddenly all these public health officials changed their mind. Now that could be perfectly reasonable — perhaps the scientific understanding and evidence changed. Right? So where is that evidence? In this article published at brownstone.org, you find a summary review of 167 studies and evidence points, “comprised of comparative effectiveness research as well as related evidence and high-level reporting. To date, the evidence has been stable and clear that masks do not work to control the virus and they can be harmful and especially to children.” The article was published in December 2021.
Another review, “Evidence for Community Cloth Face Masking to Limit the Spread of SARS‐CoV‑2: A Critical Review”, this time looking at 16 clinical studies, reached the same conclusion that masks do not help.
There are plenty of people and organisations who continue to claim that the evidence shows that masks really do work. Here’s one example, “Mask skeptics ask questions. PolitiFact answers”, that includes links to lots of studies in support of mask usefulness. Even the CDC in the US is still pumping out awful “research” that simply does not stand up to scrutiny, as outlined in this article “Mask Studies Reach a New Scientific Low Point”. The author of that article, Vinay Prasad, concluded:
“Ultimately, the CDC and NIH failed us. The agencies should have run a half-dozen masking cluster RCTs under different conditions, and for different ages. We were starving, and we needed this loaf of bread. Instead, the CDC published flawed study after flawed study. It didn’t even give us crumbs; it gave us a fistful of sand. Starving, we swallowed each grain, and begged for more. Medical leaders told us to fill our bowl before it runs out. Science lies on its deathbed.”
Mask Studies Reach a New Scientific Low Point, by Vinay Prasad
You can make your own mind up about what “The Science” is saying. My conclusion is that masks are pointless for protecting you or others against COVID. The evidence that seems to be most frequently cited by mask advocates is that masks prevent droplets from being projected by the mask wearer. It has been accepted from way before March 2020 that respiratory viruses like influenza and coronaviruses transmit primarily via aerosols, which are tiny particles that masks have no chance of trapping, and therefore I consider this to be an irrelevant point of evidence. Others argue that even if masks help a “tiny little bit” then it is our moral duty to wear one: “my mask protects you, your mask protects me”. Once again, to me this is a nonsense arguement. How can they help a “tiny little bit”? If a person is infectious, they are exhaling billions of aerosol particles. Does anyone really think that a mask trapping 100 million particles but allowing 900 million others through, has reduced risks for anyone?
Bringing things back then, to matters of trust. My issue is with the about turns made by public health professionals and politicians, when they have offered zero scientific evidence in support of the changes.
“15m jabs to freedom”
The Joint Committee on Vaccination and Immunisation (“JCVI”) published their advice on priority groups for COVID-19 jabs on 30 December 202044. This set out the plans for jabs to be prioritised for different groups, beginning with care homes and over 80s and working through groups then finally with those over 50 being eligible.
Government sources say that between 12 million and 15 million people have been identified as likely to require hospital treatment if they contract coronavirus, or be at risk of dying from it. Once this group has received the vaccine – which some officials hope could be achieved by the end of February – then the NHS would no longer be at risk of being overwhelmed if the virus spread through the greater population. That would remove the main argument for shutting the economy at a stroke.
“15m jabs to freedom”, The Daily Mail, 27 December 2020
Of course this never came to pass. Restrictions continued well beyond the point in Feb/March 2021 when this target was achieved.
“These vaccines are not appropriate for children”
In November 2020 Matt Hancock, then Secretary of State for Health and Social Care, declared in parliament that:
“This vaccine will not be used for children, it hasn’t been tested on children and the reason is, that the likelihood of children having significant detriment if they catch COVID-19 is very very low. So this an adult vaccine for the adult population.”
Matt Hancock, Secretary of State for Health and Social Care, UK Parliament, November 2020
That of course, proved not to be the case. Once again, changing direction could well be justified. What justification was given? On 4 August 2021, The Joint Committee on Vaccination and Immunisation released their advice that 16-17 year old children should be offered jabs. What was now different from Hancock’s assertion that “the likelihood of children having significant detriment if they catch COVID-19 is very very low”. The ONS data on COVID deaths shows 2 deaths in the 10-19 year old range in the whole of the UK. Two deaths. Would jabs have prevented those two tragic deaths? Who knows. How the JCVI or anyone can reach a conclusion that the benefits outweigh the potential harms for that age group, I really don’t know.
Then on 3 September 2021 the JCVI released their findings advising against jabbing of 12-15 year olds who have no underlying health conditions. Well, finally a sensible decision. Barely hours later however, the government announced that they had asked the Chief Medical Officers of the four nations to consider if there are any other factors that should be taken into account that would drive a different conclusion that in fact 12-15 year olds should be offered jabs. And lo and behold, on 13 September 2021, they reached their conclusions that it was appropriate to offer jabs to 12-15 year olds. Their main rationale was as follows (bolding by me):
On balance however, UK CMOs judge that it is likely vaccination will help reduce transmission of COVID-19 in schools which are attended by children and young people aged 12 to 15 years. COVID-19 is a disease which can be very effectively transmitted by mass spreading events, especially with Delta variant. Having a significant proportion of pupils vaccinated is likely to reduce the probability of such events which are likely to cause local outbreaks in, or associated with, schools. They will also reduce the chance an individual child gets COVID-19. This means vaccination is likely to reduce (but not eliminate) education disruption.
Universal vaccination of children and young people aged 12 to 15 years against COVID-19
So they concluded that for 12-15 year olds, who are at as close to zero risk as anyone could be without actually being at zero risk, jabs were fine as this would help prevent making school life a bit messy. This mealy-mouthed wrongthink makes me SEETHE. You only have to look at the situation in January and February of 2022 to understand what utter nonsense this non-logic always was. Up and down the country, schoolkids at all ages have been testing positive for COVID and consequently isolating for perhaps two weeks. Everybody KNEW the jabs don’t stop transmission, and that every kid in the country was probably going to get infected at some point, and therefore with isolation regulations in place, would miss some school time. This was not a decision, nor advice, that in any way, shape, or form, had the welfare of children and their health in mind. Nope, instead they pressed ahead, approving jabs for 12-15 year olds. This was of course held out to be “voluntary”, but then the NHS/Schools vaccine machine fires up, and it appears like it’s more of a “Get jabbed” command. My own personal experience of the volume and frequency of communication from the NHS about my own children and jabs bears testament to this – it was like being stalked!
Nothing on personal health
We are approaching the two year anniversary of the UK public health response to COVID. It has been apparent from very early in that response that comorbidities are a major risk factor with COVID — obesity and diabetes in particular. In that time, I don’t think I have seen a single advert or public health campaign from our public health establishment that seeks to drive a reversal in obesity in the UK population. Not one. That is beyond poor, bordering on criminal.
Throughout the COVID debacle, many have been suggesting that vitamin D supplements can play a positive role in protecting against infection and more serious disease. Many studies to look at this were criticised or debunked, and you can see why if you take a read of this article in The Daily Mail that includes summaries of a number of such studies. Most of the studies were poorly designed, or failed to account for confounding factors. And now an Israeli study pops up45, where someone had the wit to use data about vitamin D levels prior to COVID infection, and the study concluded that pre-infection deficiency of vitamin D was associated with increased disease severity and mortality. Why could the very well-funded UK public health establishment not have commissioned a competent study into the impact of vitamin D?
Behavioural manipulation
It has now no longer a secret that the government ‘nudge’ unit went to considerable efforts to stoke excessive and unnecessary levels of fear in the general public about the COVID situation. See articles “Government ‘used grossly unethical tactics to scare public into Covid compliance’ ” and “Downing Street’s controversial ‘Nudge Unit’ accused of exploiting scare tactics during Covid crisis” and “Use of fear to control behaviour in Covid crisis was ‘totalitarian’, admit scientists” in The Telegraph.
“highly questionable whether a civilised society should knowingly increase the emotional discomfort of its citizens as a means of gaining their compliance”
From open letter to the Public Administration and Constitutional Affairs Committee from 47 psychologists
Gary Sidley outlines the ethical issues with these behavioural manipulation strategies very well, in this excerpt from san article in The Critic:
We all strive to maintain a positive view of ourselves. Utilising this human tendency, behavioural scientists have recommended messaging that equates virtue with adherence to the Covid-19 restrictions, so that following the rules preserves the integrity of our egos while any deviation evokes shame. Examples of these nudges in action include: slogans such as, “Stay home, Protect the NHS, Save lives” and “Protect yourselves, Protect your loved ones”; TV advertisements where an actor tells us, “I wear a face covering to protect my mates”; the pre-orchestrated Clap for Carers ritual; ministers telling students not to “kill your gran”; and close-up images of acutely unwell hospital patients with the voice-over, “Can you look them in the eyes and tell them you’re doing all you can to stop the spread of coronavirus?”
A year of fear, Gary Sidley, The Critic, 23 March 2021
See below for examples from the government advertisement campaigns adopting these methods.




Adopting these behavioural manipulation techniques, in place of open, honest and accurate information dissemination, led me to have serious doubts about the merits and scientific basis of many of the measures the government and public health establishment were deploying. And those doubts extend to the messaging about COVID jabs.
Policies that have jumped the shark
The final item related to things that have eroded my trust, comes with examples of policies that are simply ludicrous. For a good and recent example, lets go back to schools. We have a situation in January 2022, where children are being asked to test themselves regularly, and if they test positive, to isolate at home until testing turns negative, regardless of symptoms or not. Right now, most schools are seeing very very high levels of infections (but not symptoms…).
Consider for a moment an alternative policy. One which removes testing entirely, and leaves families to determine whether their child should go to school based on their health. If they are sick, keep them at home, if not send them to school. Hardly a radical policy — that is what we have been doing in the UK for decades, prior to COVID.
At first blush, some react to this alternative policy suggestion with rage. “But, but…that could mean some children being at school infected with COVID without knowing it, and spreading it! Are you mad!?”
Think about it for a moment, though. Kids are testing positive, are not ill, and are isolating at home, and in spite of this, infection rates in the schools are sky high. If a child is susceptible to infection, then they are going to be infected very soon anyway. The only thing the current policy achieves is to guarantee that every susceptible child is out of school for an isolation period, when they inevitably test positive. What a nonsense, for a policy that was supposed to be trying to minimise school disruption!
All those jabs for kids made a big difference too, didn’t they…
F. My decision to decline – summary
A quick recap then, on my reasons for declining the jabs. Having started with an instinctive feeling that I wasn’t convinced that the jabs were a great idea, I then fairly quickly figured out that the benefit/risk trade-off for me lay heavily in the very low benefit camp. I was at very low risk from COVID. I also didn’t like the absence of long-term trials. Then as time progressed, and more data became available, I developed real concerns about the adverse effects the jabs could have. Finally, on top of all that, relentless government, social and media pressure appeared, and intensified. This, together with the various factors which eroded my trust in the government, public health and medical establishment, only served to make me more even more certain I had made the right decision for me, and in addition, that that decision had zero consequences for anyone else.
9. Closing thoughts
Various people will read this article. Some will be interested to hear why I made the choice I did, but otherwise couldn’t care less about my choice. Some will have a strong conviction that by choosing not to get jabbed, I am somehow selfish, ungrateful, and/or impinging on the health of others, who have been jabbed. To the people who hold such convictions, I invite you to have a dialogue with me, because I don’t believe any of those criticisms can fairly be levelled at me or anyone else who declined the jabs.
In very simple terms, I am not getting jabbed because:
- I am at very very low risk from COVID;
- The jabs are not fully tested and I am increasingly worried by reports of serious adverse side effects;
- I am not putting others at risk (actually I put others at less risk than the jabbed do);
- I am not a burden on the NHS, without the jab.
The jabbed are not protecting “granny”, me, each other, or the seriously sick and/or immunocompromised people in our hospitals and communities any more than I am: the jabbed can be infected and pass on the virus EVEN MORE than I can as unjabbed.
The jabbed are not “doing their bit to bring this pandemic to an end” while I am doing the opposite: the jabbed are driving spread at greater rates than the unjabbed. Which, by the way, I am not critical of — there are lots of trade-offs with these choices.
The jabbed are not “saving the NHS, because they are rarely hospitalised and don’t get seriously ill with COVID”, while the unjabbed are “flooding NHS capacity, sick only with COVID”. A huge majority (likely over 90%) of those hospitalised with COVID have already got serious illnesses, and/or are obese — that is why they end up in hospital. Almost two-thirds of those hospitalised caught COVID after they were admitted to hospital.Hospital transmission is a ‘major driver of infection that is still being ignored’
I see two potential paths here which could drive a conclusion that in fact perhaps I am selfish and damaging other people’s health. Either there are errors in the evidence I have presented in this article to support my assertions, or, I have a blind spot and I have omitted inclusion of some significant factor(s) which make a no-jab choice a toxic one. If you think either of these is the case, again please talk to me, I am more than willing to listen and be challenged.
Some may still remain unconvinced:
Right, look. I’ve read this whole article now and, you know, most of the things you’ve said, I get. Each point seems to make sense. But I just don’t buy it. You’re expecting me to believe that Chris Whitty, JVT, Boris, Hancock, Vallance, Javid, Zahawi, the people at Pfizer, AstraZeneca, Biden, Trudeau, Ardern, Morrison, the EU, the World Health Organisation, Macron, SAGE, the Queen, the Pope, Elton John, Gary Lineker, the list is endless…you expect me to believe that they are all total fuckwits who have got this all wrong? How on earth could that possibly be the case? You’ll have to give me some explanation for that.
That is a really good question. But they don’t need to be total fuckwits for it to be OK that you can choose to be jabbed and I can choose not, and that to be OK. (Quite a few on that list are total fuckwits, though.) If you want an interesting take on why things might be happening the way they are, I suggest that you read this book: Autopsy of a Pandemic, by Julius Ruechel. Eleven quid on Amazon, 276 pages, but the text size is massive so you will get through it in no time.
And now we come to my final, and most important point. Considering my valid reasons for not getting jabbed as outlined above, none of these are even necessary. There is a more fundamental reason why I can make this choice – what happens to my body is my choice and my choice alone, free from bullying, coersion and/or penalty imposed by the state. The same would be true even if there were jabs developed that actually did prevent infection and/or transmission. In these circumstances, it wouldn’t matter to anyone else whether I was jabbed or not. If you were worried, then you could get jabbed and protect yourself (or, potentially harm yourself if you experience an adverse reaction).
As for now, when my head hits the pillow I sleep easily, my conscience clear.
10. Addendum: More analysis and hypotheses
This section is VERY draft. I’m going to look at a few things:
– NHS COVID activity, by patient age
– NHS Critical Care load, by patient characteristic
– Overall pandemic response & associated policy
NHS COVID activity by patient age
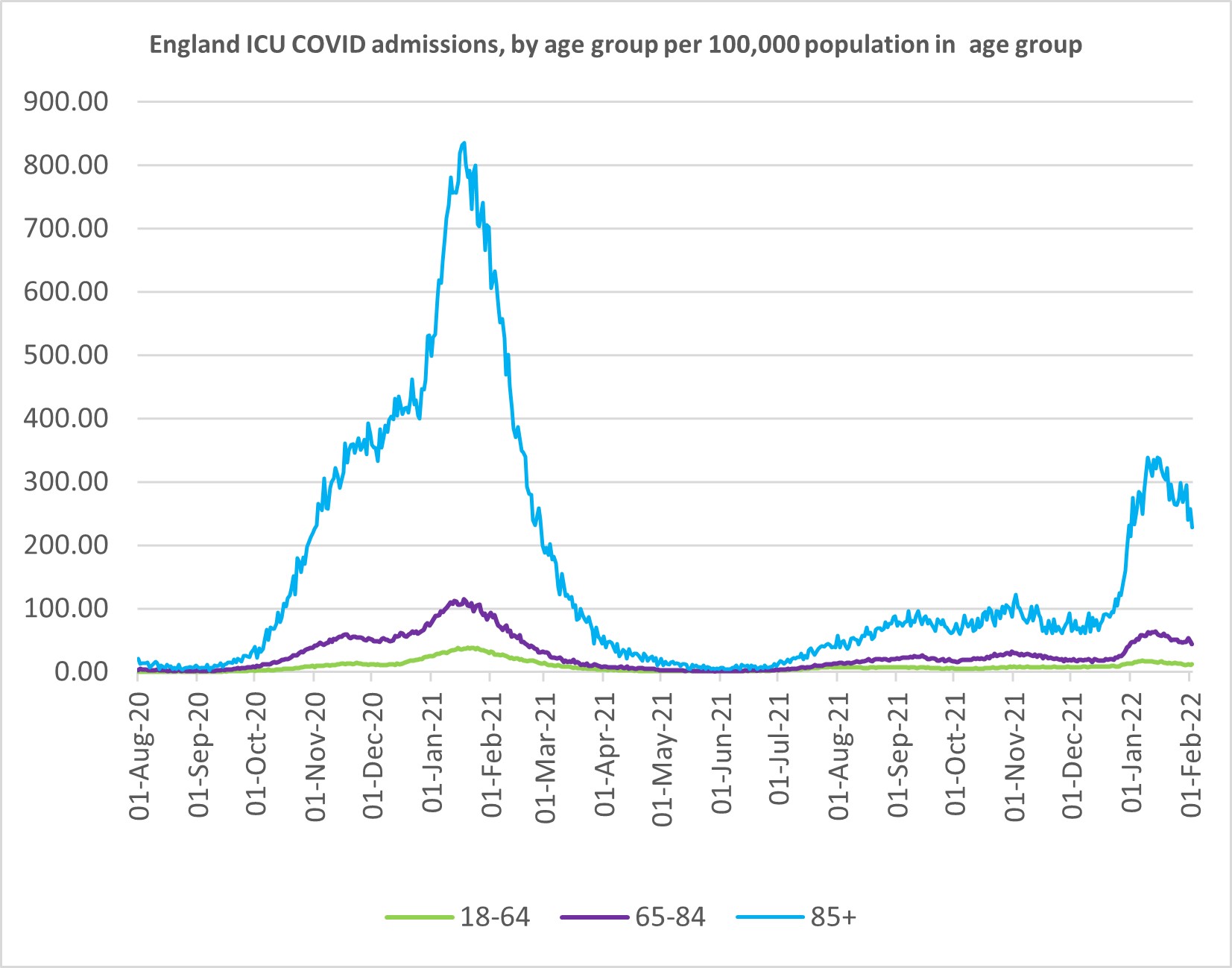

What’s the lesson? Over 65s are the main and disproportionate COVID challenge for ICU.
Aside from the March/April 2020 period, NHS ICU was most under pressure for a short period Jan/Feb 2021 with COVID-driven activity (green line in graph below).

And so when the NHS faced the most challenging phase of COVID, when the jab rollout had been going a couple of months, ICU was at capacity, with a mix of 55:45 for over-65:under-65, when over-65s comprise 20% of the adult population.
NHS Critical Care Load – Obesity
And from ICNARC, we can see that for the period 1 May 2021 to 6 Jan 2022, 49.5% of COVID ICU admissions were for patients with Body Mass Index levels of >30 which is obese, and a further 30.7% who are overweight. That means 80.2% of ICU admissions were overweight or obese.
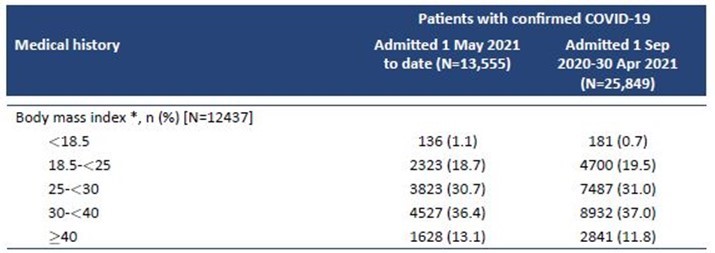
Again looking at ICNARC data for the period 1 May to 15 December 2021, we see that in both the jabbed and unjabbed cohorts of ICU admissions, each have median BMI levels of 30 which evidences the extent to which BMI is a risk factor for severe disease. If ever there was a signal that jabs for overweight and obese are a priority, it is this data.
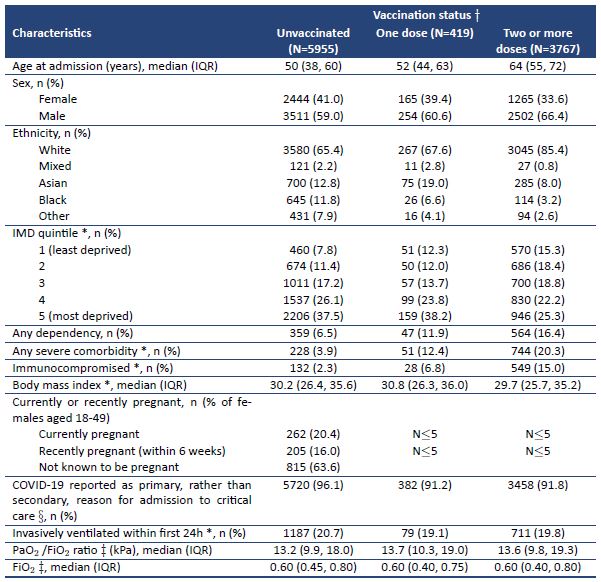
Turning then to deaths in England, and COVID. The graph below shows this from March 2020 to January 2022, for both 60+ and under 60. Where is the line for the under 60s I hear you ask?? You need to look very carefully – it’s almost flat against the x-axis. All those jabs for <60 age group — what were they for again?
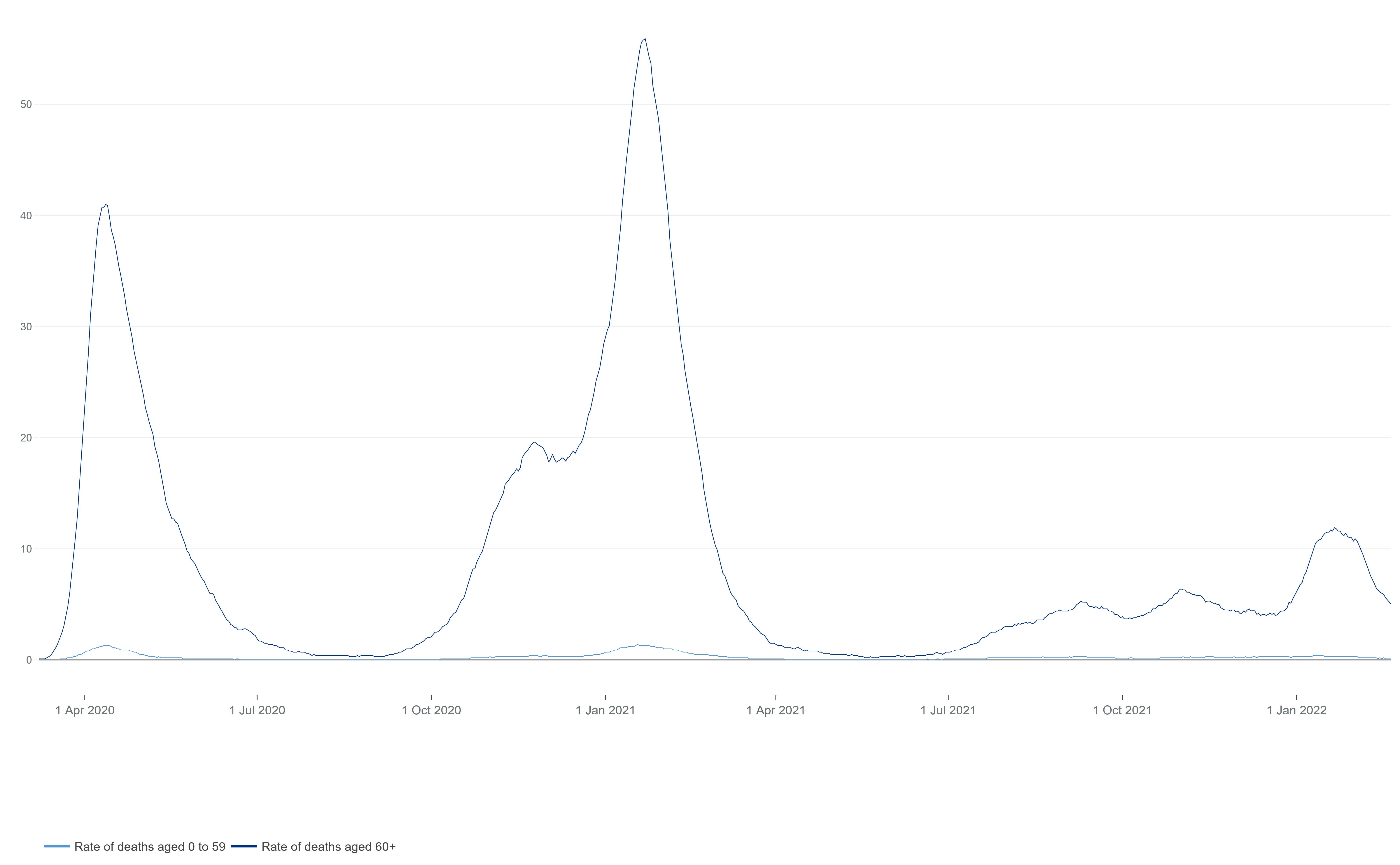
And thus all the above is, in a nutshell, what gives the underpinning to my assertion that universal vaccination was wholly unnecessary. Offer jabs to the elderly (65+), and to those in high risk categories (obese, diabetic, immunocompromised). This would have freed up significant resource for the NHS to divert to patient care.
Overall pandemic response
Key points:
– lockdowns do nothing useful to prevent spread or infection
– masks do nothing. full stop.
– social distancing makes no difference to spread
– nor do contact-limiting policies, like rule-of-6, tier 1/2/3/4 etc
– clear from early on that elderly and vulnerable are 1,000x more at risk than most
– pushing to discover a vaccine is a fine objective
– however no vaccine for a coronavirus was ever going to stop infection or transmission
– by the time jabs arrived, also clear that obesity and diabetes were huge risk factors for hospitalisation and/or death
– the early focus for jab deployment was rightly elderly and vulnerable
– the virus is seasonal…by start of April 2021, infection levels had collapsed versus January peaks
– unexpected counter-seasonal uptick in infection rates from July 2021. Consistent with a jab that induces infection! (By then, 65% of 18+ population had been jabbed)
– ICU attendance May – Dec 2021 saw 80% COVID patients being overweight or obese
– situation then gets concerning in early 2022…1 or 2-dose people see higher rates of hospitalisation/death than the unjabbed. 3+ doses continues to see lowest rates of hospitalisation/death
Overall Conlusion
– elderly, obese/overweigh, diabetic getting jabbed, reduces the NHS burden
– non-pharma interventions were pointless
– vaccinating the healthly <65 was a waste of money, effort, and diverted scarce health resource from patient care, and very likely put those people at risk of adverse side effects
– the impact on healthcare and wellbeing as a consequence of poor policy choices is going to be horrific, and long lasting. This includes but not limited to:
- suicides and mental heath damage caused by lockdowns and anti-contact policies
- child learning and development trashed by lockdowns, anti-contact policies and mask mandates
- failure to detect and treat severe illnesses, cancer, hypertension, caused by a fixation on COVID
- trashing of small businesses, especially in hospitality sector, as a result of restrictions, ruining livelihoods
- https://www.sciencemuseum.org.uk/objects-and-stories/medicine/smallpox-and-story-vaccination#what-is-vaccination
- https://www.sciencemuseum.org.uk/objects-and-stories/medicine/smallpox-and-story-vaccination#edward-jenner-and-the-smallpox-vaccine
- https://www.sciencemuseum.org.uk/objects-and-stories/medicine/smallpox-and-story-vaccination#the-science-behind-vaccination
- The Case Against Vaccination (1896) by Walter Hadwen
- Extracts from “LEICESTER: Sanitation versus Vaccination” By J.T. Biggs J.P.
- Vaccination: A Mythical History ~ by Roman Bystrianyk and Suzanne Humphries MD. (2013)
- Clinical Issues: Smallpox Vaccine: The Good, the Bad, and the Ugly. Edward A. Belongia and Allison L. Naleway. Clin Med Res 2003 1:87-92; doi:10.3121/cmr.1.2.87
- “Disease Mitigation Measures in the Control of Pandemic Influenza”. DocumentCloud. November 2006.
- Smallpox: the basics. Mark K Slifka, Jon M Hanifin. Dermatologic Clinics, Volume 22, Issue 3 (2004)
- Geeky Medics – Immune Response
- Parts of the Immune System, Children’s Hospital of Philadelphia
- https://www.historyofvaccines.org/content/articles/different-types-vaccines
- https://www.healthline.com/health-news/leaky-vaccines-can-produce-stronger-versions-of-viruses-072715
- SARS-CoV-2 Vaccines Based on the Spike Glycoprotein and Implications of New Viral Variants
- Distinguishing features of current COVID-19 vaccines: knowns and unknowns of antigen presentation and modes of action
- https://www.medrxiv.org/content/10.1101/2021.08.24.21262415v1
- Protection and waning of natural and hybrid COVID-19 immunity. Yair Goldberg, Micha Mandel, Yinon M. Bar-On, Omri Bodenheimer, Laurence Freedman, Nachman Ash, Sharon Alroy-Preis, Amit Huppert, Ron Milo. medRxiv 2021.12.04.21267114; doi: https://doi.org/10.1101/2021.12.04.21267114
- https://www.israelnationalnews.com/news/309762 “natural” immunity from recovery outperforms vaccinated immunity in covid-19
- https://www.healthline.com/health-news/study-finds-hybrid-or-super-immunity-against-covid-19-provides-most-protection
- COVID-19 vaccine surveillance report, Week 39, 2021
- COVID-19 vaccine surveillance report, Week 5, 2022
- Transmission potential of vaccinated and unvaccinated persons infected with the SARS-CoV-2 Delta variant in a federal prison, July—August 2021
- Vaccinated and unvaccinated individuals have similar viral loads in communities with a high prevalence of the SARS-CoV-2 delta variant Kasen K. Riemersma, Brittany E. Grogan, Amanda Kita-Yarbro, Gunnar E. Jeppson, David H. O’Connor, Thomas C. Friedrich, Katarina M. Grande. medRxiv 2021.07.31.21261387; doi: https://doi.org/10.1101/2021.07.31.21261387
- https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(21)00648-4/fulltext
- “Autopsy of a Pandemic”, Julius Ruechel, pp 189-193
- “Autopsy of a Pandemic”, Julius Ruechel, pp 189-193
- “Autopsy of a Pandemic”, Julius Ruechel, pp 196-198
- “Autopsy of a Pandemic”, Julius Ruechel, p 198
- This chicken vaccine makes its virus more dangerous
- https://journals.plos.org/plosbiology/article?id=10.1371/journal.pbio.1002198
- Antibody-dependent Enhancement (ADE) and Vaccines
- “Autopsy of a Pandemic”, Julius Ruechel, pp 202-205
- “Autopsy of a Pandemic”, Julius Ruechel, pp 186-187
- Vaccines and Related Biological Products Advisory Committee Meeting, FDA, December 10, 2020
- Bed Availability and Occupancy Data – Overnight
- COVID-19 Hospital Activity
- https://www.eugyppius.com/p/of-all-covid-patients-in-the-icu
- CDC study finds about 78% of people hospitalized for Covid were overweight or obese
- ICNARC report on COVID-19 in critical care
- Diaz GA, Parsons GT, Gering SK, Meier AR, Hutchinson IV, Robicsek A. Myocarditis and Pericarditis After Vaccination for COVID-19. JAMA. 2021;326(12):1210–1212. doi:10.1001/jama.2021.13443
- Epidemiology of Acute Myocarditis/Pericarditis in Hong Kong Adolescents Following Comirnaty Vaccination
- Myocarditis after BNT162b2 mRNA Vaccine against Covid-19 in Israel
- https://www.england.nhs.uk/statistics/statistical-work-areas/covid-19-vaccinations/
- Joint Committee on Vaccination and Immunisation: advice on priority groups for COVID-19 vaccination
- Pre-infection 25-hydroxyvitamin D3 levels and association with severity of COVID-19 illness